Clinical Pathology Case Study: Severe hyperglobulinemia in a dog
Background information
| Age: | 10 years |
| Sex: | Female spayed |
| Species: | Canine |
| Breed: | Retriever |
| History: | Weight loss, recent onset of lethargy and epistaxis |
Physical exemination
- A physical exam revealed that there were no significant findings.
Laboratory results and interpretation
A chemistry panel and a CBC were performed. Relevant findings include:
Chemistry
| Proteins: | 116 | (55-75) | g/L |
| Albumin: | 14 | (27-39) | g/L |
| Globulin: | 102 | (24-40) | g/L |
Hematology
| Hematocrit: | 0.31 | (0.38-0.57) | L/L |
| Reticulocytes: | 35.3 | (10-110) | 10E9/uL |
| Platelets: | 296 | (143-448) | 10E9/uL |
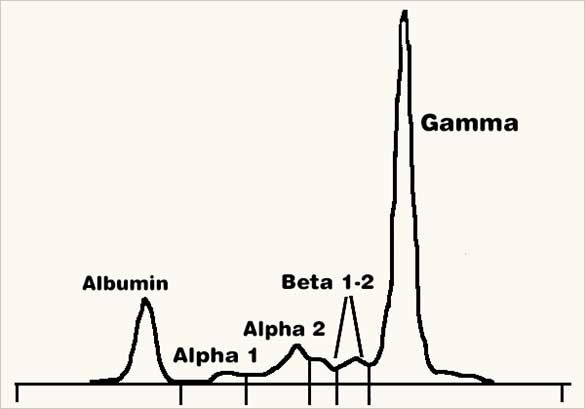
Considering the marked hyperglobulinemia, serum protein electrophoresis was then performed. The electrophoretogram located at the top of the page was obtained.
Interpretation: The most likely diagnosis is an immunoglobulin-secreting neoplasm, such as multiple myeloma or lymphoma.
Discussion
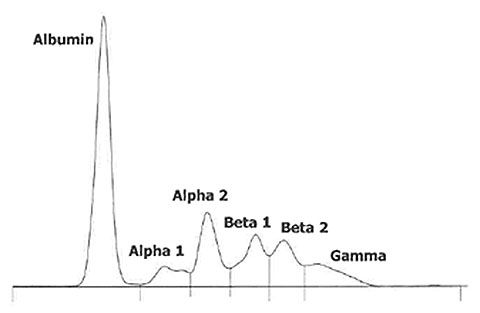
Electrophoresis of serum proteins separates the major blood protein fractions into 6 categories (see fig. 2 - Normal Electrophoresis). Alpha- and beta-globulins mostly include positive and negative acute phase proteins, whereas gamma-globulins are comprised of immunoglobulins (mostly IgG).
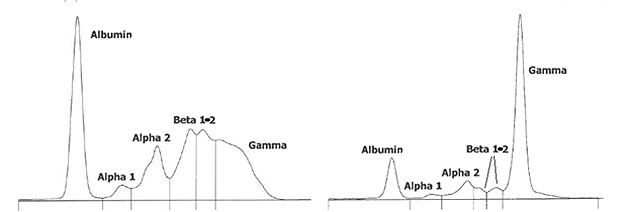
The gamma region is most informative. When hyperglobulinemia occurs as a result of antigenic stimulation, a large variety of immunoglobulin types are synthesized targeting various epitopes. These different immunoglobulins have different migration patterns, and they spread broadly upon electrophoresis. This results in the formation of one or many, short, broad and/or coalescing peaks in the gamma region: a polyclonal gammopathy (see Fig.3 – Polyclonal Gammopathy). On the other hand, in multiple myelomas (malignant tumor of plasma cells) and in occasional cases of lymphoma, the neoplastic cells all originate from the same abnormal cell and they all synthesize and secrete the same immunoglobulin chain with the same migration pattern, resulting in a monoclonal gammopathy (see. Fig. 4 – Monoclonal Gammopathy).
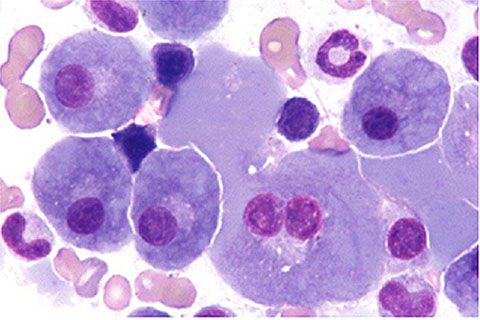
Our patient’s electrophoresis is consistent with a monoclonal gammopathy. A multiple myeloma or lymphoma is therefore highly likely. However, note that monoclonal gammopathies are not absolutely pathognomonic for neoplasia, as the medical literature contains occasional case reports where unusual antigenic stimulation lead to monoclonal gammopathy, including cases of ehrlichiosis. Further investigation for multiple myeloma and lymphoma is therefore warranted. Ehrlichiosis should be ruled out by performing a Snap 4DX. Evaluation of internal organs and peripheral lymph nodes should then be considered. Note that the diagnosis of multiple myeloma requires that at least 2 of the following 4 criteria should be documented: a monoclonal gammopathy on serum protein electrophoresis, osteolytic lesions, Bence-Jones proteinuria (i.e. monoclonal immunoglobulin chains in the urine), and/or bone marrow plasmacytosis (see. Fig. 5 – Bone Marrow Plasmacytosis - Cytology).
Despite a normal platelet count, our patient is exhibiting epistaxis, suggesting a coagulopathy of primary hemostasis (which is generally platelet-related). This is a common complication in cases of severe hyperglobulinemia due to proteins coating platelets and interfering with their normal function. Severe hyperglobulinemia can also lead to blood hyperviscosity, which interferes with blood flow in smaller vessels. This may cause hypertension, ophthalmic lesions, and neurological signs.
About the author
Sébastien Overvelde, DVM, MSc, DACVP
A native of Sherbrooke, Quebec, Dr. Overvelde received his DVM from the University of Montreal in 1998 and then worked in a small-animal practice in Newport News, Virginia, for 3 years. He returned to the University of Montreal to complete a residency in clinical pathology and a master’s degree in veterinary science. Dr. Overvelde attained American College of Veterinary Pathologists board certification in 2004 and joined IDEXX at the Montreal laboratory in November of the same year.He became head of clinical pathology for Canada in 2008.
Dr Overvelde lives in Laval, Quebec, with his wife and two daughters. His family also includes two cats, a guinea pig and many fish. In his spare time, he enjoys karate, kayaking, cooking, and genealogy research.
Should you have any questions about this case or wish to discuss the diagnosis in greater detail, please do not hesitate to contact the author.
View clinical pathology case studies
NEW: Dermatophytosis in a dog, by Caroline Piché, DMV, IPSAV, MSc, Diplomate ACVP
Anaplasmosis in a dog, by Julie Webb, DVM, DACVP
Blastomycosis in a dog, by Julie Webb, DVM, DACVP
Cryptococcus in a dog, by Carrie Flint, DVM, DACVP
Cutaneous mycobacteriosis (Leprosy) in a cat, by Natalie Kowalewich, DVM, DACVP
Demodex in a dog, by Brittney Fierro, DVM, DACVP
Feline infectious peritonitis in a cat, by Heidi Peta DVM, MVSc, DACVP
Mammary fibroepithelial hyperplasia in a young cat, by Emmeline Tan, DVM, DVSc, DACVP
Microvascular dysplasia in a dog, by Cathy Monteith DVM, MVSc, DACVP
Severe hyperglobulinemia in a dog, by Sébastien Overvelde, DVM, MSc, DACVP
References
Feldman BF, Zinkl JG, Jain NC. Schalm’s Veterinary Hematology. 5th Edition. Lippincott Williams & Wilkins, 2000.
Withrow SJ, MacEwen EG. Small Animal Clinical Oncology. 3rd Edition. WB Saunders Company, 2001..
All case studies were prompted by real submissions to IDEXX Canada pathologists at one of our reference laboratories.
To protect the confidentiality of our customer and clients, the background information in each case has been slightly modified.